Just as a reminder, the conduction system is as follows:
Conduction System of the Heart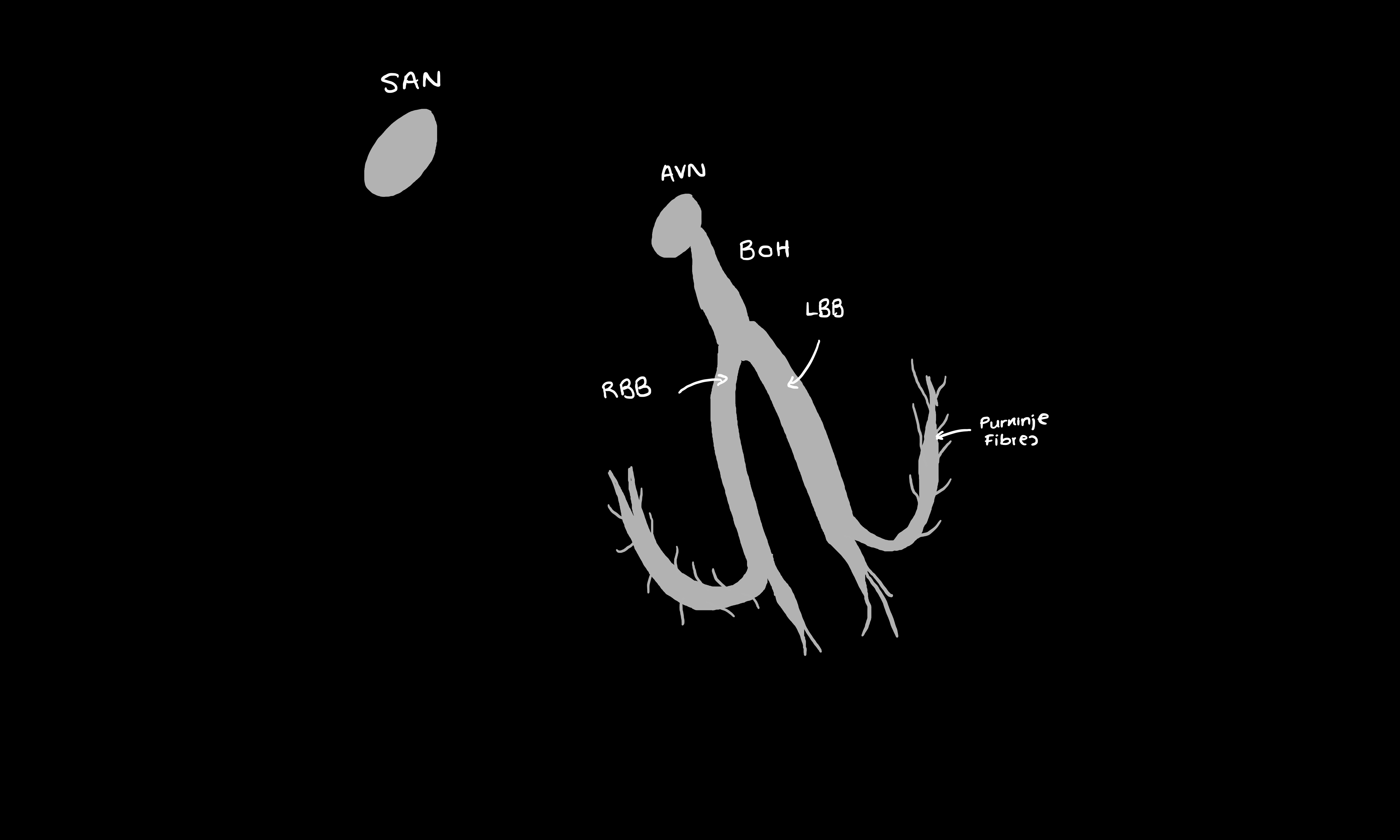
Atrioventricular block, also called heart block, occurs when there is a disease in the AVN which results in a prolonged delay in the conduction of depolarisations of the SAN towards the ventricles.
In second degree heart block, there are some depolarisations of the SAN that fail to be conducted through to the ventricles. There are two types of second-degree heart block.
Mobitz Type I (Wenckebach)
Mobitz Type II
Advanced Heart Block
In third degree heart block, no SAN depolarisations conduct through to the ventricles, and the ventricles are relying on an ‘escape rhythm’ i.e. rhythm which is not arising from the SAN. Usually, this rhythm is generated by the AVN, bundle of His or Purkinje fibres and beats slower than the atria.
In this case, there is no pattern with the PR interval and there is no relationship between the P waves and QRS complexes because the atria and ventricles are beating independently.
First-degree and Mobitz I may be simple benign variants, whilst Mobitz II and third-degree heart block usually indicate a more serious underlying cause. This can be:
The symptoms of heart block can vary depending on the degree of heart block. For example, first degree heart block may cause no symptoms at all. Some patients with higher degrees of heart block may complain of lightheadedness, chest pain, dyspnoea, fatigue, and confusion.
Sometimes, patients can present with syncope which occurs suddenly without warning. These are sometimes known as Stokes Adams attacks, which are characterised by sudden collapse followed by a short period of unconsciousness and a rapid recovery. They are usually caused by a third-degree heart block but other causes do exist.
12-lead ECG is the main investigation of choice for diagnosis.
Some types of AVN heart block i.e. first-degree and Mobitz I usually do not require treatment, especially if patients are asymptomatic. If patients do develop symptoms, drugs which block the AVN should be stopped e.g. beta-blockers. For especially severe symptoms however, treatment may be necessary.
Higher grade heart blocks such as Mobitz type II or third-degree heart block usually warrant management with cardiac pacing. NICE recommends that patients with symptomatic bradycardia as a result of atrioventricular block receive dual-chamber cardiac pacing. If the patient is particularly frail, has specific co-morbidities, or has continuous atrial fibrillation in addition to atrioventricular block, single chamber pacing of the ventricle may be more appropriate.
https://www.nice.org.uk/guidance/ta88/chapter/1-guidance
Davidson's Principles of Medicine 23rd Edition
