A collection of signs and symptoms which occur due to excessive cortisol levels in the body.
Pathophysiology
-
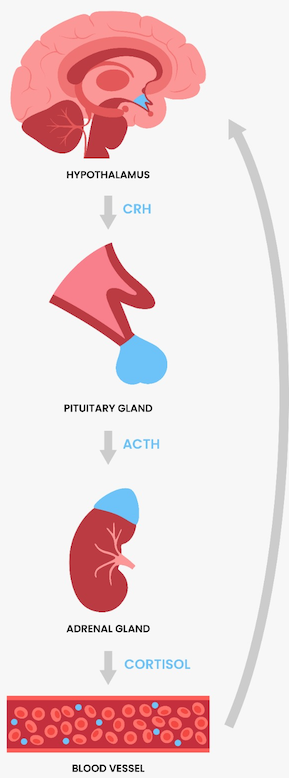
The hypothalamus secretes corticotropin releasing hormone (CRH) from the paraventricular nucleus.
-
CRH reaches the anterior pituitary via the hypophyseal portal system and stimulates ACTH secretion.
- ACTH stimulates cortisol release and androgen production by the adrenal cortex. The zona fasciculata of the adrenal gland is responsible for producing glucocorticoid hormones, including cortisol.
- ACTH and melanocyte-stimulating hormone (MSH) share the same precursor, proopiomelanocortin (POMC). MSH is responsible for stimulating the production and release of melanin from melanocytes. Thus, in cases of raised ACTH, patients may have hyperpigmentation.
- Cortisol has a negative feedback effect on CRH and ACTH release.
- Cortisol is a glucocorticoid. Its main actions include:
| Upregulation | Downregulation |
| Gluconeogenesis | Protein synthesis |
| Protein breakdown | Response to infection |
| Fat deposition | Healing |
| Potassium excretion | |
| Sodium retention | |
| Increased neutrophils | |
7. Cortisol has a diurnal variation whereby it is highest in the morning, usually at around 8-9am, and is lowest in the evenings i.e. around midnight.
8. It is excreted as urinary free cortisol
Copyright Medic in a Minute 2022
HPA Axis
Cushing's syndrome is the collection of signs and symptoms associated with excess levels of glucocorticoid hormones, including cortisol - remember, a syndrome is just a description of signs and symptoms.
Cushing's disease, however, is the specific condition where. you have a pituitary adenoma over-secreting ACTH, resulting in excessive levels of cortisol.
Causes
ACTH Dependent: Excess ACTH
ACTH Independent: Normal ACTH
| ACTH Dependent | ACTH Independent |
| Cushing’s disease: over-secretion of ACTH by a pituitary adenoma | Excessive use of exogenous steroids |
| Ectopic secretion of ACTH e.g., by a small cell lung carcinoma | Adrenal adenoma or carcinoma producing cortisol |
| Ectopic CRH secretion (rare) | |
Clinical Features
General
- Rounded, moon face
- Buffalo hump
- Hypertension
- Fatigue
- Weight gain
- Impaired glucose tolerance/diabetes
Skin
- Acne
- Hirsutism
- Purple striae on abdomen
- Easy bruising and thin skin
- Hyperpigmentation: Only in ACTH-dependent causes
Musculoskeletal
- Proximal muscle wasting resulting in proximal myopathy
- Impaired glucose tolerance or diabetes mellitus
- Osteoporosis
Behavioural
- Mood symptoms: Irritability, depression, psychosis
- Insomnia
- Reduced libido
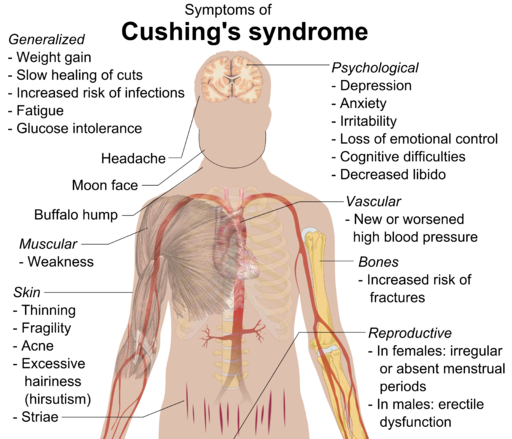
Mikael Häggström, CC0, via Wikimedia Commons
Clinical Features of Cushing's Syndrome
Investigations
Bedside
Bloods
- FBC, LFT, TFT: Baseline/rule out differentials.
- U&E: Excess cortisol can upregulate mineralocorticoid effects resulting in hypokalaemia
- Serum ACTH: To localise the disease
- Serum glucose/HbA1c: Impaired glucose tolerance
Imaging
- Chest x-ray: If suspecting a paraneoplastic syndrome
- CT Abdomen and Pelvis: If considering an adrenal mass
- Pituitary MRI: If suspecting pituitary adenoma
Special Tests
- 24-hour urinary cortisol: Since cortisol is excreted in the urine, its amount can be measured over a 24-hour period.
- 1mg overnight dexamethasone suppression test:
- Patient takes 1mg of synthetic glucorticoid (dexamethasone) at 10pm.
- At 9am, the patient comes to clinic and cortisol is measured.
- Dexamethasone should suppress cortisol to <50nmol/L via a negative feedback loop on the HPA axis.
- Higher levels of dexamethasone are needed to suppress Cushing’s disease (pituitary adenoma). Ectopic tissues do not respond to higher levels of dexamethasone which helps localise disease.
- 48-hour low dose dexamethasone suppression test:
- Works similarly to the 1mg overnight test but has a lower rate of false positives
- Midnight and morning salivary cortisol: Lowest level of cortisol is at midnight and highest is at 9am in the morning.
Localising the Tumour
- If high cortisol, but low ACTH: Primary adrenal cause and need to do adrenal imaging
- If high cortisol, but high ACTH: Suggests ACTH dependent pathology. You'd then have the task of localising what part of the body is secreting the ACTH - is it the pituitary (Cushing's disease), the hypothalamus (ectopic CRH), or is it a paraneoplastic syndrome?
Management
Medical Management
Metyrapone and ketoconazole are examples of two drugs which can be used to lower cortisol. They both work by inhibiting enzymes involved in cortisol synthesis.
However, it is important to consider that these are not definitive treatments.
Surgical Management
- Trans-sphenoidal surgery: To remove pituitary tumours. This can be coupled with radiotherapy if needed.
- Laparoscopic surgery: For removal of adrenal tumours