When there is damage to the left or right bundle branches in the cardiac conducting system, it can result in right bundle branch blocks (RBBB) or left bundle branch blocks (LBBB).
Conduction System of the Heart
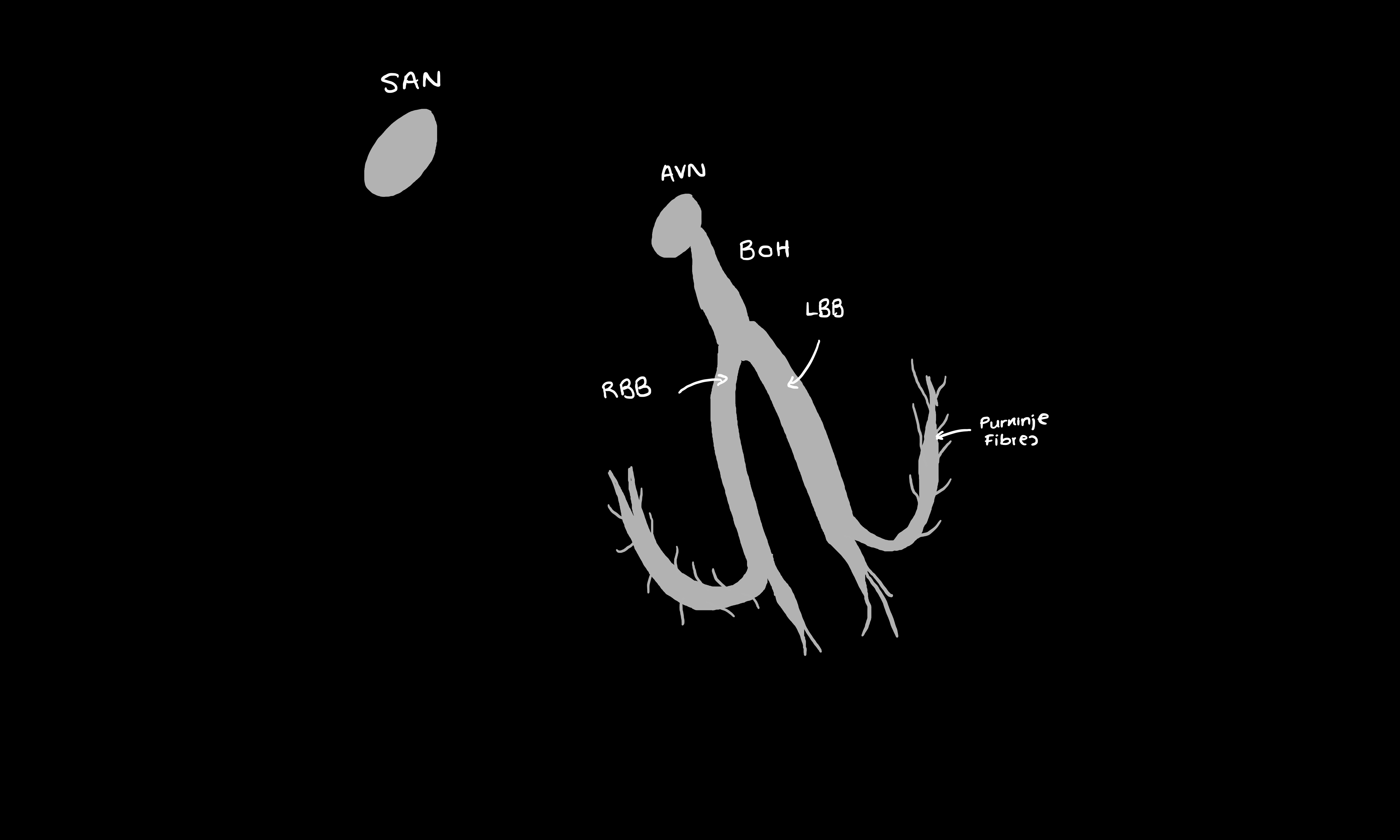
The conduction system of the heart is as follows:
Sinoatrial node (SAN) > Atrial depolarisation > Atrioventricular node (AVN) > Bundle of His > Left and right bundles (LBB/RBB) > Purkinje Fibres > Ventricular depolarisation
Copyright Medic in a Minute 2023
Conduction System of the Heart
If the left and right bundle branches become damaged, depolarisation will end up going through the myocardium as opposed to the faster conductive tissue. This results in a delayed conduction of ventricular depolarisation, which broadens the QRS complex as it’s taking longer to depolarise the entirety of the ventricular muscle.
The left bundle branch actually splits into left anterior and posterior fascicles. If only one of these fascicles is damaged, it is known as a hemiblock. It does not cause a wide QRS complex, but an axis deviation will occur.
- Left anterior hemiblock = Left axis deviation
- Left posterior hemiblock - Right axis deviation
If there is a RBBB and a left hemiblock (i.e. one of the fascicles is affected), it is known as a bifasicular block.
If both the right and left bundle branches become blocked, it results in a third-degree (complete) heart block.
Causes
- LBBB: Can occur if the cardiac tissue becomes stretched as it can damage the conduction tissue, cardiac scarring or infiltration of the conduction system
- Dilated cardiomyopathy i.e. through stretching of the conductive system
- Coronary artery disease
- Hypertension
- Myocardial infarction
- Sarcoidosis
- RBBB
- If the QRS complex is not wide, but there is a RBBB pattern, it may be a normal variant
- Right ventricular hypertrophy
- Right ventricular strain e.g. pulmonary embolism
- Coronary artery disease
Electrophysiology
Leads and Directions on an ECG
- We're going to walk through the ECG findings - if you understand what's happening, it'll be easier to interpret the ECG.
- Leads V1 and V6 are the main leads used to diagnose a bundle branch block, with V1 showing the view of the right ventricle and V6 showing the view of the left ventricle.
- Remember, when depolarisation is moving towards a lead, it causes an upward deflection and when it moves away it causes a downward deflection.
Just a recap:
- Q wave: This is a downwards deflection
- R wave: This is an upwards deflection
- S wave: This is the downwards deflection following the R wave
The QRS Complex
- There are two main occassions where QRS complexes tend to be broad:
- When depolarisation starts within the ventricles rather than going through the conductive system
- A bundle branch block. By definition, for a bundle branch block to exist, the QRS needs to be broad i.e. >120 ms/> 3 small squares
Normal Physiology
If you remember that the septum depolarises from left towards the right, it'll make everything a bit easier. It does this via the left branch from the Bundle of His, depolarising the septum in that specific direction.
RBBB ECG
ECG Morphology - Depolarisation Explained
RBBB: The right bundle is dysfunctional, so your right side conduction will be dysfunctional.
- Septum Depolarisation:
- As the left bundle is in tact, the septum still depolarises from the left to the right, as is normal.
- V1 (View of the R side of the heart): R wave (upward deflection), as depolarisation moves towards the right i.e. V1
- V6 (View of the L side of the heart): Q wave (downward deflection), as depolarisation moves away from the left i.e. V6
- Left Ventricular Depolarisation:
- The left ventricle then depolarises first, rather than simultaneous depolarisation of the ventricles (latter is normal physiology).
- V1 (View of the R side of the heart): S wave (downward deflection), as depolarisation moves away from the right
- V6 (View of the L side of the heart): R wave (upward deflection), as depolarisation moves towards teh left
- Right Ventricular Depolarisation
- The right ventricle then depolarises, but slowly due to a blocked right bundle branch.
- V1 (View of the R side of the heart): R wave (upward deflection), as depolarisation again moves towards the right
- V6 (View of the L side of the heart): S wave (downward deflection that follows an R wave), as depolarisation moves away from the left
ECG Morphology - rSR' and QRS Pattern Explained
- V1: View of the Right Heart: rSR'
- R wave: First, depolarisation moves from the left, towards the right i.e. towards V1, resulting in an upwards deflection, or an R wave.
- S wave: Then, depolarisation spreads through the left ventricle i.e. away from V1, resulting in an S wave.
- R' wave As the right bundle branch is blocked, it takes longer for depolarisation to spread throughout the right ventricle. Therefore, once the right ventricle eventually depolarises, it causes a second R wave in V1, called R'.
- V6: View of the Left Heart: qRs
- Q wave: As depolarisation moves from the left towards the right i.e. away from V6, it causes a downward deflection, or a Q wave.
- R wave: Depolarisation then spreads through the left ventricle i.e. towards V6, causing an upward deflection, or R wave.
- S wave: Once the right ventricle eventually catches up and depolarises, the depolarisation of course moves away from the left ventricle and thus V6, which causes an S wave (downward deflection after an R wave).
Because the RSR looks sort of like an M, and the QRS looks a little like a W, you can remember a RBBB with MaRRoW.
LBBB ECG
ECG Morphology - Depolarisation Explained
LBBB: The left bundle is dysfunctional, so your left side conduction will be dysfunctional.
- Septum Depolarisation:
- The left bundle is now disrupted, so the septum will not depolarise from left to right, but from right to left.
- V1 (View of the R side of the heart): Q wave (downward deflection) as depolarisation moves away from the right i.e. V1
- V6 (View of the L side of the heart): R wave (upward deflection), as depolarisation moves towards the left i.e. V6
- Right Ventricular Depolarisation
- The right ventricle now depolarises first, down the faster and in-tact conduction mechanism.
- V1 (View of the R side of the heart): R wave (upward deflection), as depolarisation moves towards the right
- V6 (View of the L side of the heart): S wave (downward deflection following an R wave), as depolarisation moves away from the left
- Left Ventricular Depolarisation
- The left ventricle now depolarises, but much more slowly due to the disrupted fast conduction mechanism.
- V1 (View of the R side of the heart): S wave (downward deflection following an R wave), as depolarisation moves away from the right side of the heart
- V6 (View of the L side of the heart): R wave (upward deflection), as depolarisation moves towards the left.
ECG Morphology - QRS and rSR Pattern Explained
- V1: QRS
- Q wave: As depolarisation moves from the right towards the left, it causes a downward deflection in V1 (depolarisation moves away from V1)
- R wave: This signifies depolarisation of the right ventricle – since the muscle mass of the right ventricle is smaller than the left, it causes a smaller upward deflection (R wave) since the depolarisation is moving towards lead V1.
- S wave: Eventually, the left ventricle depolarises – as this is a depolarisation moving away from V1, it causes a downward deflection in this lead i.e. an S wave.
- V6: RSR
- R wave: As depolarisation moves from the right towards the left, it causes an upward deflection in V6 (depolarisation moves towards V6).
- S wave: This is the depolarisation of the right ventricle, causing a small downward deflection in V6 as the depolarisation is moving away.
- R wave: This is the depolarisation of the left ventricle, which moves towards V6 thus causing an upward deflection.
The QRS in a LBBB looks a little like a W (the S wave is a lot deeper than the preceding R wave), whilst the RSR complex looks sort of like an M. Thus, WILLIAM, can be used to remember a LBBB pattern. Furthermore, a LBBB is associated with T wave inversion in the lateral leads i.e. V5, V6, I and vL.
Why does the QRS for a RBBB look different for the QRS in the LBBB?
You need to consider what the R and S waves are showing. In the RBBB, the R wave in V6 signifies depolarisation of the left ventricle, which has a large muscle mass and therefore produces a higher amplitude. The S wave signifies the depolarisation of the right ventricle – it is downwards since the depolarisation is moving away from V6, and it is smaller because the right ventricle has less muscle mass, thus producing a smaller amplitude deflection.
In the LBBB, the R wave in V1 signifies depolarisation of the right ventricle (upward deflection as depolarisation moves towards V1). However, the small muscle mass of the right ventricle only produces a smaller amplitude deflection. The S wave signifies the depolarisation of the left ventricle (downward deflection as the depolarisation moves away from V1). This wave is ‘deeper’ since there is a larger muscle mass in the left ventricle.
Thus, although both have ‘QRS’ morphology, they look slightly different.
References
https://www.ncbi.nlm.nih.gov/books/NBK482167/
https://www.ncbi.nlm.nih.gov/books/NBK507872/
Hampton JR. The ECG Made Easy 9th edition.
https://ecg.utah.edu/lesson/3
https://www.sciencedirect.com/topics/medicine-and-dentistry/heart-depolarization