Benign Paroxysmal Positional Vertigo (BPPV) is a disorder characterised by brief, intense episodes of vertigo triggered by specific head movements.
Pathophysiology
The Vestibular System
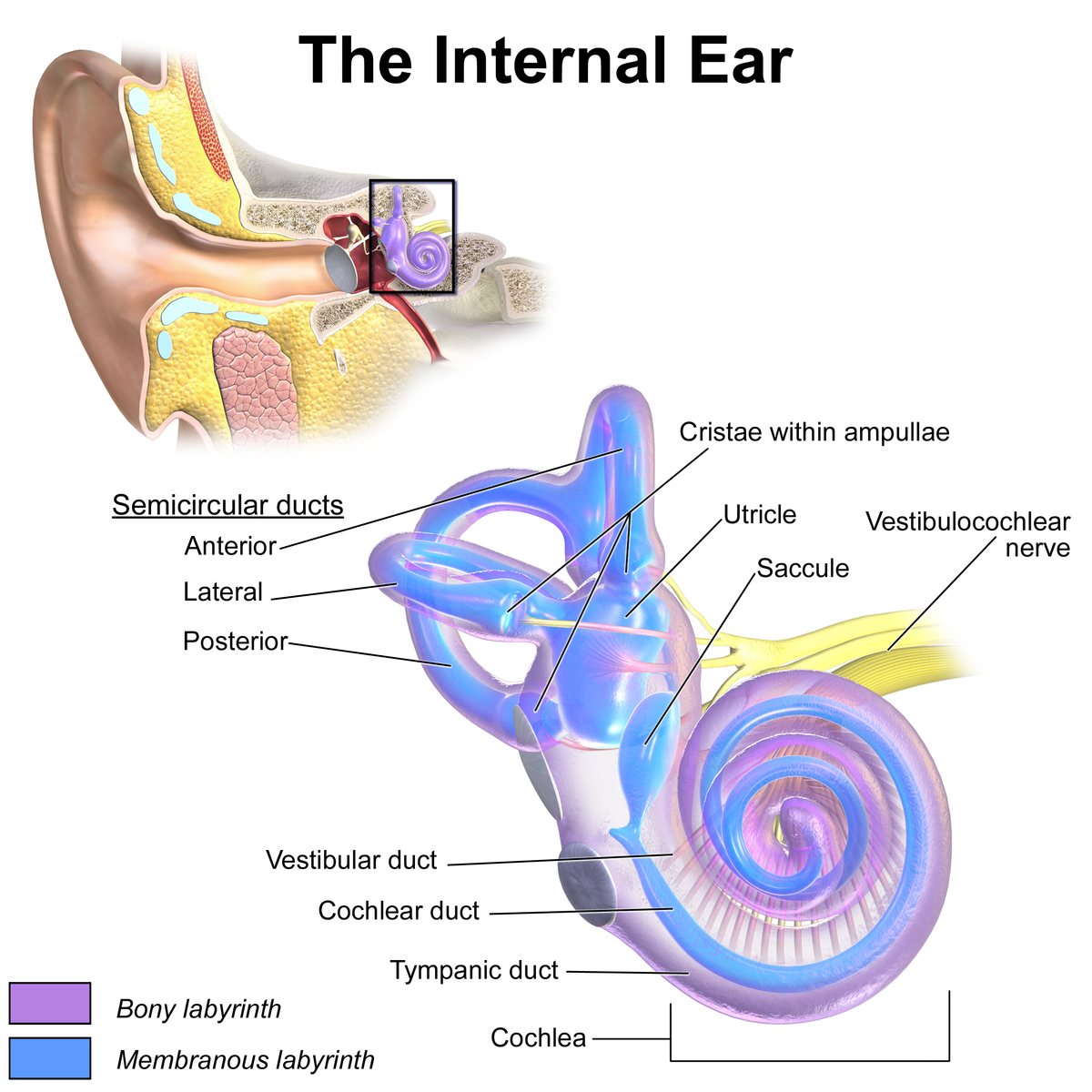
- The inner ear can be split into two key parts – the cochlea (hearing), and the vestibular system (balance). We’ll talk a bit more about the vestibular system.
- The vestibular system is made up of 3 semi-circular canals. Each of these form enlarged areas at the end called the ampullae.
- Followed by this you have the two otolith organs – the utricle and the saccule, and then finally the cochlea which is the thing that looks like a snail shell.
Semi-Circular Canals
- The 3 semi-circular canals sit in 3 planes, 45 degrees to each other, and detect movements in those respective planes.
- Horizontal/Lateral: This detects movements in the transverse plane i.e., when you move your head from side to side (shaking your head no).
- Posterior: This detects movements in the coronal plane i.e., when you touch your ear towards your shoulder so tilting movements of the head.
- Superior: This detects movements in the sagittal plane i.e., up and down movements so when you nod your head up and down.
- At the end of each semi-circular canal is a widening known as the ampulla. The ampulla has hair cells which have stereocilia on them, which extends into something called the cupula, a membrane that attaches to the top of the ampulla.
- The semi-circular canals contain endolymph, a fluid similar to neuronal intracellular fluid. When the head moves in a particular plane, the endolymph in the corresponding semi-circular canal moves.
- This in turn, moves the cupula and stereocilia, resulting in neuronal firing and detection of head movement.
BruceBlaus. When using this image in external sources it can be cited as:Blausen.com staff (2014). "Medical gallery of Blausen Medical 2014". WikiJournal of Medicine 1 (2). DOI:10.15347/wjm/2014.010. ISSN 2002-4436., CC BY 3.0 , via Wikimedia Commons
Inner Ear Anatomy
Otolith Organs
- The otolith organs (utricle and saccule) help the brain detect gravity and linear acceleration. The utricle is responsible for detecting horizontal motion, whilst the saccule detects vertical motion.
- The utricle and saccule are made up of macula tissue, which is basically a bunch of support cells with hair cells. The hair cells have stereocilia, which extend into a gel-like membrane called the otolithic membrane.
- On top of the otolithic membrane are otoconia, which are crystals of calcium carbonate.
- When the head is moved, the otoconia membrane moves which results in bending of the stereocilia that extend into it, causing firing of neurones and thus the detection of head movement.
BPPV
- In BPPV, it is thought that otoconia become dislodged within the semi-circular canals. At a resting, neutral position of the head, these do not move. When the head moves however, these become displaced, resulting in signals incoherent with head position.
- This is what results in vertigo seen in BPPV.
- Most commonly, the posterior semi-circular canal is affected, followed by the horizontal/lateral canal, and finally the anterior canal.
Risk Factors
- Head injury
- Females
- Low vitamin D
- Migraine
- Age ≥ 65
Clinical Features
- Dizziness, particularly on movements of the head. Usually short, transient episodes of <1 minute
- Nausea/vomiting
Investigations
Bedside
- Dix-Hallpike Manoeuvre: This is used in the diagnosis of BPPV.
- Ask the patient to sit upright on a bed. You’re going to lay the patient supine later in the manoeuvre such that their head will hang slightly off the end of the bed, so make sure they’re sitting in a way that allows for that.
- You then ask the patient to turn their head 45 degrees to one side. The side you move their head to is the side you are testing.
- You ask the patient to keep their head still, and to keep their eyes open throughout the manoeuvre.
- Whilst supporting the head and neck, the patient is then quickly moved from a seated position to the supine position, with their head hanging off the end of the bed and in extension of around 30 degrees.
- The eyes are then observed for any nystagmus – you should wait around 30 seconds as there can be a latent period before the onset of nystagmus. A positive test is the presence of nystagmus +/- vertigo.
- Nystagmus in Dix-Hallpike is specifically torsional/rotatory (interchangeable terms)– the eye will rotate slightly, essentially having both a vertical and diagonal component. The rotation will be in the direction of the ear that is facing downward.
- The patient is then sat up, and the test is repeated on the other side.
- ECG: Rule out pre-syncope as a possible cause of dizziness – ensure you clarify with patients what they mean by dizziness i.e. ensure they do not mean to say lightheadedness.
Differential Diagnosis
- Vestibular neuronitis/labyrinthitis: An acute onset of severe vertigo secondary to inflammation and infection of the inner ear.
- Meniere’s disease: Associated with tinnitus, hearing loss, and fullness of the ear.
- Posterior stroke
Management
- Watchful waiting: Most people’s symptoms will self-resolve
- Epley manoeuvre: This is a particle repositioning manoeuvre and essentially aims to dislodge the otoconia causing the underlying BPPV.
- Similar to Dix-Hallpike, the patient begins in a seated position, and will end up with their head extended 30 degrees over the end of the bed, so ensure the patient is positioned properly.
- First, the patient’s head is turned 45 degrees to the affected side.
- The patient is laid backwards, ensuring their head is kept still and supported. This is maintained for 30 seconds.
- The head is then rotated 90 degrees to the opposite side.
- Semont manoeuvre: Similar to the Epley
- Brandt-Daroff exercises: These are particle repositioning exercises that can be done at home by the patient independently.
- Efficacy of Particle Repositioning Techniques: The Epley, Semont, and Brandt-Daroff are all types of particle repositioning techniques. A paper by Gupta et al found an improvement in 90%, 73%, and 50% of patients following those exercises respectively.
- Driving: Patients should not drive whilst experiencing vertigo. The DVLA advises patients with “liability to sudden and unprovoked or unprecipitated episodes of disabling dizziness” should inform the DVLA and stop driving.
References
https://pubmed.ncbi.nlm.nih.gov/32776833/
https://openstax.org/books/anatomy-and-physiology-2e/pages/14-1-sensory-perception
https://cks.nice.org.uk/topics/benign-paroxysmal-positional-vertigo/management/management/
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6401006/#:~:text=Results%20of%20Dix–Hallpike%20indicate,improved%20with%20Brandt–Daroff%20exercises.